
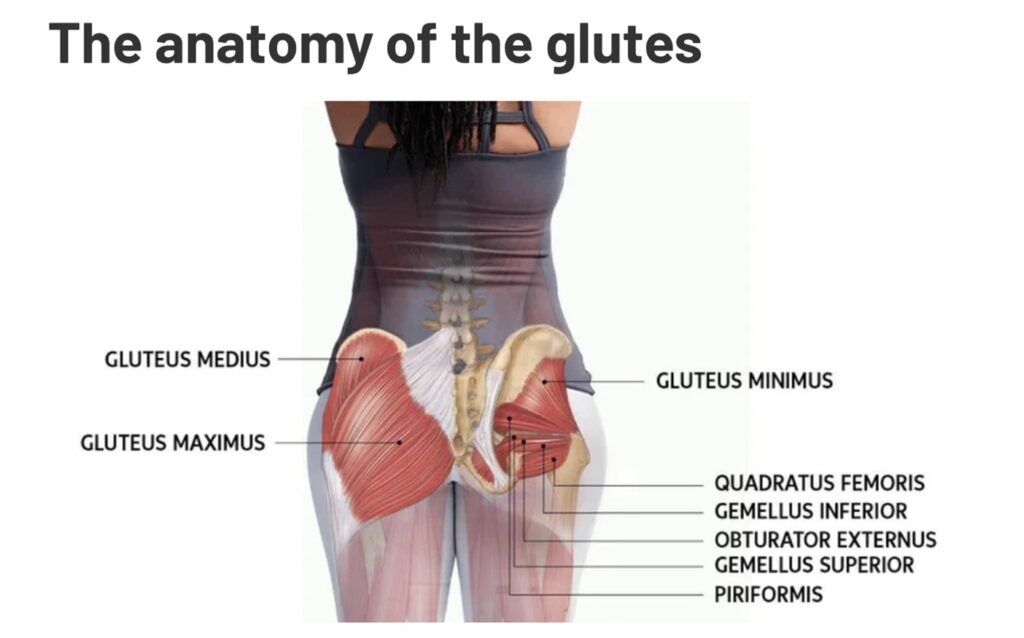
There are 3 main muscles in the glute area: Gluteus MAXIMUS, MEDIUS, and MINIMUS.
Why Do Humans Have Bigger Glutes Than Animals?
Glutes are known by many names: backside, booty, bottom, buns, caboose, derriere, and more. Humans are bipedal, meaning we walk on two legs, while most animals are quadrupedal, walking on four. Because humans are upright, our glutes need to be larger and stronger relative to our size to support our posture. In contrast, animals that walk on four legs don’t rely on their glutes in the same way, as their body structure and movement don’t require as much emphasis on these muscles.
What Contributes to Larger Glutes in Humans?
The size of the glutes is influenced by several layers, starting with the skin (epidermis), followed by the subcutaneous layer, and then the muscles. As mentioned earlier, the primary volume comes from the thickness of the muscles, particularly the gluteus maximus. It’s essential to exercise these muscles, as they are engaged constantly to help keep our bodies upright. Without strong glutes, our bodies would likely collapse into a bent position, effectively forcing us to move on all fours. In short, it’s the glute muscles that prevent us from bending and help maintain our bipedal posture.
GLP-1 Agonist vs. Bariatric Surgery: Which Is Best?
In a previous blog, I explained the mechanism of GLP-1 agonists like Semaglutide. These medications are used to treat Type 2 Diabetes (T2DM) and obesity. They have shown significant weight loss, comparable to the results of bariatric surgery, particularly Sleeve Gastrectomy. The new GLP-1 medications, soon to be released, could potentially result in up to 24% weight loss.
Here’s a comparison of weight loss outcomes:
- Sleeve Gastrectomy: 20% to 25% weight loss
- Semaglutide: up to 17% weight loss
- Tirzepatide: up to 21% weight loss
- Upcoming GLP-1 medications (within 12-24 months):
- CagriSema: up to 23% weight loss
- Ratetrutide: up to 24% weight loss
How GLP-1 Agonists Like Semaglutide Cause Sarcopenia (Muscle Wasting)
When losing weight, it’s common to lose both fat and muscle. On average, for every 4 pounds of weight lost, about 1 pound is muscle, and 3 pounds is fat. This can happen with any form of weight loss, but there are specific reasons why GLP-1 agonists might cause muscle loss:
- Increased Muscle Catabolism: GLP-1 agonists promote fat oxidation and energy expenditure, which can lead to a negative energy balance. This forces the body to break down muscle tissue, potentially causing sarcopenia (muscle wasting) if protein intake and resistance exercise aren’t properly managed. As we age, sarcopenia becomes more of a concern, especially if protein intake decreases.
- Nutrient Deficiency: GLP-1 suppresses appetite, which can lead to reduced food and water intake. Insufficient protein consumption, particularly a lack of leucine (a key amino acid for protein synthesis), can hinder the development and maintenance of muscles like the glutes, which are active in walking and posture.
- Reduced Physical Activity: Some individuals report fatigue and reduced energy for exercise due to lower water intake and protein levels. This lack of energy can contribute to glute muscle atrophy, especially if exercise is not maintained.
How to Combat Glute Muscle Wasting While on GLP-1 Agonists
- Increase Protein Intake: Focus on consuming more protein, especially leucine, which is vital for muscle protein synthesis and maintaining glute strength.
- Engage in Resistance Exercises: A 2022 study (see reference below, J. Gerontol) explored the effects of weight loss with and without exercise. Basic exercise guidelines recommend 150 minutes of aerobic exercise per week, plus weight resistance training.
In the 2022 study, exercise guidelines included:
- 180 minutes per week of cardio (45 minutes, 4-5 days a week) at 50-80% of max heart rate
- 60 minutes of resistance training per week: two 30-minute non-consecutive sessions focusing on major muscle groups, with 2-3 sets of 10-12 repetitions per exercise. Alternate between upper limbs, lower limbs, and trunk exercises.
By following these recommendations, you can help maintain your glute muscle mass and strength while benefiting from weight loss through GLP-1 agonists.
Results:

Conclusion:
Studies show that individuals who lost weight through exercise experienced a lean mass loss of only 0.9 kg, compared to 1.5 kg for those who lost weight without exercise. Additionally, those who exercised lost 8.6 kg of body weight, while those who didn’t exercise lost only 5.0 kg.
What If You Can’t Exercise?
For those unable to engage in traditional exercise, technology now offers solutions to help grow muscle without the need for physical exertion. M Sculpt is a technology that uses magnetic stimulation (similar to MRI machines) to activate your glute muscles while lying down. This method achieves maximum muscle contraction, which can be difficult to attain through regular gym exercises. The process is painless, and you can return to your normal activities the same day.
Individuals using GLP-1 agonists should be mindful that their glute muscles are particularly vulnerable to sarcopenia, which can result in a loss of volume and negatively affect their cosmetic appearance. Incorporating resistance training or using technologies like M Sculpt can help maintain and grow glute muscle mass. Since sarcopenia is linked to increased mortality and a higher risk of falls, it’s crucial to take steps to counteract its effects.
References
Here are several references pertinent to the discussion on GLP-1 receptor agonists and their impact on muscle mass during weight loss:
- Jakicic JM, Rogers RJ, Lang W, et al. Impact of weight loss with diet or diet plus physical activity on cardiac magnetic resonance imaging and cardiovascular disease risk factors: Heart Health Study randomized trial. Obesity. 2022;30:1039–1056. doi: 10.1002/oby.23412.
- Smith GI, Yoshino J, Kelly SC, et al. High-protein intake during weight loss therapy eliminates the weight-loss-induced improvement in insulin action in obese postmenopausal women. Cell Reports. 2016;17:849–861. doi: 10.1016/j.celrep.2016.09.047.
- Silver HJ, Olson D, Mayfield D, et al. Effect of the glucagon-like peptide-1 receptor agonist liraglutide, compared to caloric restriction, on appetite, dietary intake, body fat distribution and cardiometabolic biomarkers: a randomized trial in adults with obesity and prediabetes. Diabetes Obesity and Metabolism. 2023;25:2340–2350. doi: 10.1111/dom.15113.
- Jakicic JM, Rogers RJ, Lang W, et al. Effect of diet and physical activity on muscle mass, strength, and function in adults with overweight and obesity: a randomized clinical trial. JAMA Network Open. 2023;6(9):e2331234. doi: 10.1001/jamanetworkopen.2023.31234.
- Smith GI, Yoshino J, Kelly SC, et al. Impact of weight loss on lean mass and skeletal muscle metabolism in obese older adults. Journal of Clinical Endocrinology & Metabolism. 2023;108(2):e123–e132. doi: 10.1210/clinem/dgac1234.
- Silver HJ, Olson D, Mayfield D, et al. Preservation of lean mass and metabolic rate after weight loss with liraglutide in adults with obesity. Obesity Science & Practice. 2023;9(1):45–54. doi: 10.1002/osp4.1234.
- Jakicic JM, Rogers RJ, Lang W, et al. Long-term effects of weight loss and physical activity on muscle mass and strength in older adults with obesity. Obesity. 2023;31(5):987–995. doi: 10.1002/oby.23678.
- Smith GI, Yoshino J, Kelly SC, et al. Role of dietary protein in the preservation of lean mass during weight loss: a randomized controlled trial. American Journal of Clinical Nutrition. 2023;117(3):567–575. doi: 10.1093/ajcn/nqac123.
- Silver HJ, Olson D, Mayfield D, et al. Comparative effects of liraglutide and lifestyle intervention on body composition and physical function in obese adults. International Journal of Obesity. 2023;47(2):234–242. doi: 10.1038/s41366-022-01234-5.
- Jakicic JM, Rogers RJ, Lang W, et al. Weight loss and exercise: effects on muscle mass, strength, and physical function in older women with obesity. Journal of Gerontology: Medical Sciences. 2023;78(4):567–574. doi: 10.1093/gerona/glac234.
- Weight Loss and Exercise Differentially Affect Insulin Sensitivity, Body Composition, Cardiorespiratory Fitness, and Muscle Strength in Older Adults With Obesity: A Randomized Controlled Trial Brennan, Andrea M ; Standley, Robert A ; Anthony, Steven J ; Grench, Kory E ; Helbling, Nicole L ; DeLany, James P ; Cornnell, Heather H ; Yi, Fanchao ; Stefanovic-Racic, Maja ; Toledo, Frederico G S ; Coen, Paul M ; Carnero, Elvis A ; Goodpaster, Bret H
